

How Is An Anterior Inferior Tibiofibular Ligament Repaired
view
all
clinics
MRI Web Clinic — August 2014
Accessory Anterior Inferior Tibiofibular (Bassett's) Ligament
Leon R. Toye, M.D.
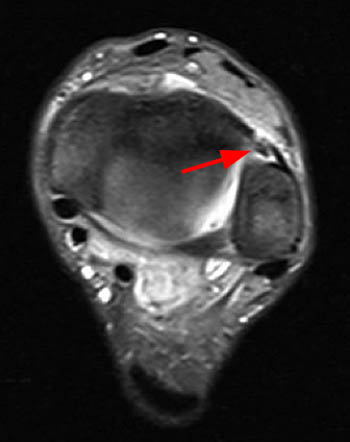
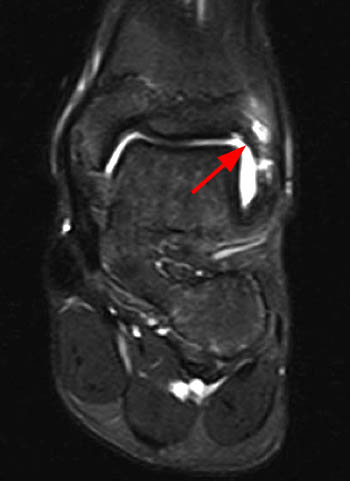
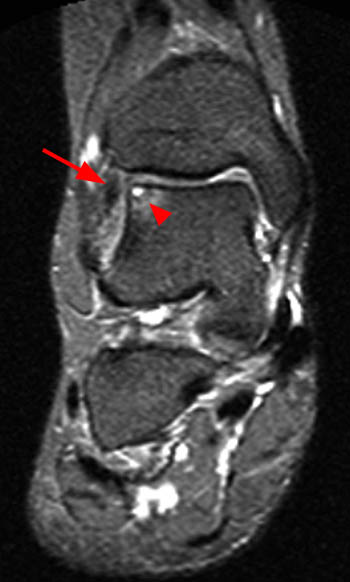
Clinical History: A 16 twelvemonth-old female presents with chronic anterolateral ankle pain and a history of injury one year prior. Oblique centric proton density-weighted (1A) and coronal (1B) and sagittal (1C) T2-weighted fat-suppressed images are provided. What are the findings? What is your diagnosis?
 1a
1a
 1b
1b
 1c
1c
Oblique axial proton density-weighted (1A) and coronal (1B) and sagittal (1C) T2-weighted fat-suppressed images demonstrate an abnormally thickened accessory anterior inferior tibiofibular (Bassett's) ligament (arrows), surrounded past prominent fluid and/or synovitis within the anterolateral ankle gutter.
Diagnosis
Thickened accessory anterior inferior tibiofibular (Bassett's) ligament, contributing to anterolateral impingement.
Introduction
Anterolateral ankle impingement is a common crusade of chronic ankle pain, typically following inversion injuryi , 2 , 3. Multiple factors may contribute to pain from anterolateral impingement, including synovitis, hyalinized scar tissue, and chondral injury of the talar dome3. A bottom known contributing factor to anterolateral impingement is a thickened accessory anterior junior tibiofibular ligamenti, iv. This accessory ligament is an anatomical variant present in the almost ankles1, 4 , 5, which may get sprained and pathologically thickened in the setting of inversion injury, resulting in impingement and balmy residual inductive instability1, iii.
Anatomy
The distal tibiofibular articulation is composed of a ligamentous complex including the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), and the interosseous ligament. Posteriorly, a transverse ligament is also present, which coalesces with the PITFL to form the then called tibial slip or intermalleolar ligamentsix.
The AITFL is a flat band typically attaching to the distal tibia approximately 5 mm above the articular surface, anterior to the interosseous ligament, descending obliquely, attaching to the anterior aspect of the lateral malleolus4,3 (Figure 2). The length ranges from 12-22 mm, thickness from i.v-three mm, and width from 9-22 mm (at the tibial zipper) to 7-12 mm (at the fibular attachment)4.
A distal separate ligament or fascicle of the AITFL has been described, located just distal to the AITFL, the accessory inductive inferior tibiofibular ligament. The structure was originally described by Nikolopoulos in a Greek 1982 thesis but never published in the English literature7 , 4. Basset et al. get-go described the construction in the English literature, and also start described an associated impingement upon the talar dome, , found at both arthroscopy and cadaveric dissections. Bassett described the structure every bit an accessory fascicle to the AITFL, present in most man ankles (found in 10/eleven cadavers). Nikolopoulos later performed boosted cadaveric studies concluding the structure was a distinct separate ligament from the AITFL due to the presence of an intervening fibrofatty septumfour, 3.
The accompaniment anterior junior tibiofibular ligament (also published in the radiology literature equally "Bassett's ligament")8 runs parallel and distal to the AITFL, also attaching to the tibia and fibula (Figure 3). The distal attachment of Bassett'south ligament approximates the fibular attachment of the anterior talofibular ligament (ATFL)ix , 3. The length ranges from 17-22 mm, thickness from one-2 mm, and width from iii-5 mm9, 3.
 two
two
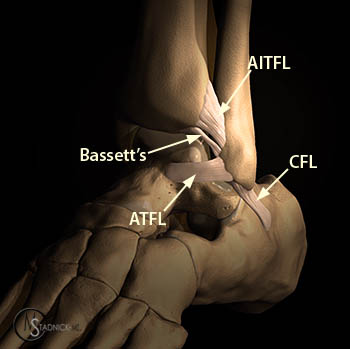
Graphic illustration demonstrates the normal relationships of the anterior inferior tibiofibular ligament (AITFL), accessory anterior inferior tibiofibular ligament (Bassett'due south ligament), inductive talofibular ligament (ATFL), and calcaneofibular ligament (CFL).
 3
3
Cadaveric specimen shown in the lateral orientation demonstrates the relationships of the AITFL (black arrow), Bassett's ligament (white arrow), and the ATFL (blue pointer) and their sites of attachment on the lateral malleolus (asterisk). Photograph courtesy of Emily N. Vinson, Medico, Duke Academy Medical Center.
Pathology
Repetitive microtrauma may result in hypertrophied synovial tissue and fibrosis within the anterolateral gutter, contributing to hurting and anterolateral impingement10 , 11 , 12. In avant-garde cases, the mechanical impingement may mold tissue into a hyalinized "meniscoid lesion", originally described by Wolin et al13 , 4 (Figure iv).
 iv
iv
Graphic analogy demonstrates hypertrophied synovial tissue and fibrosis within the anterolateral gutter, contributing to anterolateral impingement.
Basset et al. postulated that post-traumatic anterolateral hyperlaxity, due to an injured ATFL, results in anterior extrusion of the talar dome with dorsiflexion, contacting the accompaniment junior fascicle of the AITFL, with more pressure and friction1, 3. This results in thickening of the accessory AITFL, contributing to anterolateral impingement (Figure five). Of notation, the AITFL may still exist normal in the presence of a pathologic accompaniment AITFL1, 8.
 v
v
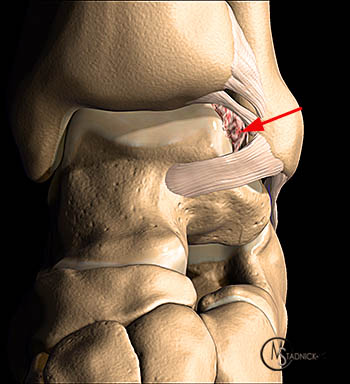
Graphic illustration demonstrates an abnormally thickened Bassett's ligament, surrounded by synovitis/inflammation, contributing to anterolateral impingement.
Akseki et al. postulated that variations in the width, length, and obliquity of the accessory AITFL fascicle may result in pathologyv. Wider and longer fascicles are potentially at greater risk. A fibular attachment bespeak far from the joint level was also thought to result in greater gamble.
Several authors written report the clan of talar dome chondral chafe with the presence of a pathologic accessory AITFL. Anterior and anterolateral talar dome articular cartilage abrasion has been reported to be nowadays in 82.9%ix, 17%5, and 71%1 of cases of an abnormal accessory AITFL. Presumably the abnormally thickened accessory AITFL contacts the superolateral talar dome, resulting in the cartilage chafethree (Figure six).
 6
6
A coronal T2-weighted image demonstrates an anterolateral talar dome chondral lesion and subchondral bone edema (arrowhewad), in conjunction with a thickened Bassett'southward ligament (arrow).
Imaging
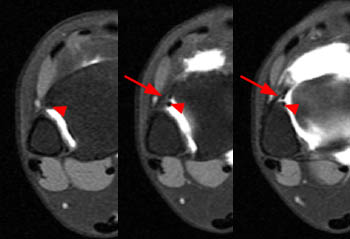
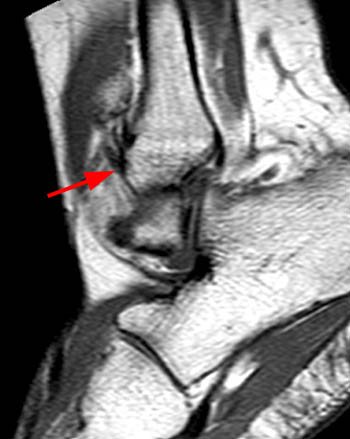
Subhas et al. reported Bassett's ligament to be visible in all iii standard MR imaging planes, seen most unremarkably (89%) with sequential axial images8. Due to the anatomic orientation of Bassett'due south ligament, coronal imaging is often easiest to visualize the low signal fibers paralleling the grade of the AITFL, and separated by a band of higher signal (Figure 7). Centric images are useful to identify the fibular attachment located junior and slightly medial to the AITFL fibular attachment (Figure 8). Sagittal images again demonstrate Bassett's ligament inferior to the fibular attachment of the AITFL, at or below the apex of the anterior fibular contour (Figure ix). The tibial attachment of Bassett's ligament may be less conspicuous due to blending of fibers with the AITFL.
 7
7
A coronal T2-weighted fatty-suppressed prototype showing the oblique orientation of Bassett's ligament (arrow), paralleling the AITFL, separated by a thin band of increased signal.
 8
8
Centric fatty-suppressed T1-weighted arthrographic images progressing from superior (left) to inferior (right) demonstrate Bassett's ligament (arrowhead) attaching to the fibula, medial and inferior to the AITFL (pointer).
 9a
9a
 9b
9b
Sagittal T1 (Figure 9) and fat-suppressed proton density-weighted (Figure 9b) images in two different patients demonstrating the fibular attachment of Basset's ligament, located inferior to that of the AITFL, located at or inferior to the to the noon of the fibular contour (arrow). Effigy 10 as well demonstrates an abnormally thickened ATFL (arrowhead).
Due to the modest size of Bassett's ligament, determining normal from pathologic thickening can be difficult, with greater degrees of thickening having greater chances of beingness pathologic. In the study of Subhas et al., a Bassett's ligament thickness of greater than 3 mm was 89% specific for subsequent arthroscopic pathology8.
Irregular or nodular low betoken tissue between the AITFL and ATFL has a loftier correlation with anterolateral scarring and/or synovitis11. The absence of a fluid filled recess betwixt the anterolateral soft tissues and the anterior surface of the fibula has also been described as a sign of scarring and/or synovitis10, 11 (Figure 10). If present, osseous fragments or spurs may likewise contribute to anterolateral impingement (Figure 11).
 10a
10a
 10b
10b
Axial T2-weighted fatty-suppressed (Figure 10a) and axial T2-weighted non fatty-suppressed (Effigy 10b) images in different patients demonstrate ill-defined intermediate to low bespeak within the anterolateral gutter, consistent with synovitis and scarring (arrows).
 11a
11a
 11b
11b
Osseous contributions to anterolateral impingement. An axial T2-weighted image (Effigy 11a) demonstrates an ununited avulsion ossification in the anterolateral gutter (pointer). An axial T1-weighted image (Figure 11b) in a different patient demonstrates prominent osseous spurs along the anterior joint (arrows).
Direction
If conservative treatment fails, arthroscopic debridement is considered a safe and effective method to confirm and care for anterolateral impingement[14 Urgüden M, Söyüncü Y, Ozdemir H, Sekban H, Akyildiz FF, Aydin AT. Arthroscopic treatment of anterolateral soft tissue impingement of the talocrural joint: evaluation of factors affecting upshot. Arthroscopy. 2005 Mar;21(three):317-22.]. Diagnostic ankle arthroscopy is first performed in a systematic mode, evaluating for synovitis, scar tissue, a thickened Bassett'southward ligament, and chondromalacia of the talar dometwo. Debridement of hypertrophic scar tissue is performed. If present, an abnormally thickened Bassett's ligament is excised1, fourteen. Loose bodies may be removed. Chondroplasty is also performed, as necessarytwo. Postoperatively, the patient is placed in a soft dressing for a few days. Early on physical therapy is begun shortly after, involving gentle movement, musculus strengthening, proprioceptive balancing exercises, and weight-bearing as tolerated15. Factors that negatively bear upon consequence include chondral lesions of the talar dome, associated syndesmotic lesions, and new inversion injuries after surgery15.
 12
12
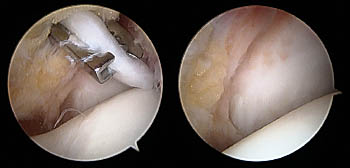
Intraoperative images demonstrate arthroscopic removal of a thickened Bassett'due south ligament (same patient as the Figure 1 MRI). The left paradigm demonstrates a thickened Bassett's ligament (white band of tissue) surrounded by a surgical "biter". The paradigm on the right is post-resection. The smooth surface on the bottom of the images represents the talar dome. The white surface behind Bassett'southward ligament is the lateral malleolus. Images courtesy of Shay Tenenbaum, Doctor, Chris Royer, Md, and James Brodsky (Baylor Academy Medical Centre, Dallas TX).
Conclusion
An accessory anterior inferior tibiofibular (Bassett's) ligament is an anatomical variant within about ankles. An injured Bassett's ligament may result in pain due to mild anterior instability (allowing slight anterior translation of the talus) and anterolateral impingement. A pathologically thickened Bassett'south ligament and other causes of anterolateral impingement tin can be demonstrated with preoperative MRI. Awareness of an abnormal Bassett's ligament, scar tissue, and associated talar dome chondral lesions can be useful in pre-operative planning.
Acknowledgments
Thanks to:
- Shay Tenenbaum, MD, Chris Royer, MD, James Brodsky, MD (Baylor University Medical Center, Dallas TX)
- Jeffrey Willers, Doctor, Lauren Erickson, PA-C, Rick Willard (Aristocracy Orthopaedic, Nashville, TN)
- Emily Vinson, Doc (Duke University Medical Middle, Durham NC)
for aid with images and support with this web dispensary.


Source: https://radsource.us/accessory-anterior-inferior-tibiofibular/
Posted by: daviscound1991.blogspot.com
0 Response to "How Is An Anterior Inferior Tibiofibular Ligament Repaired"
Post a Comment